New or worsening floaters may be a sign of the following
- posterior vitreous detachment
- vitreous hemorrhage
- retinal tear
- retinal detachment
- inflammation
- benign age-related changes
The only way to distinguish between the above entities is to undergo a careful, dilated retinal examination by an experienced eye doctor.
What is the Retina?
- If the eye were a camera, the retina would be the film of that camera
- The retina is a thin sheet of nerve cells that lines the inside back wall of the eye
- Light travels through the eye and ultimately reaches photoreceptors, the light-sensitive cells in the retina
- The signal from the photoreceptors then travel along the optic nerve to the brain, where the signals are interpreted as vision
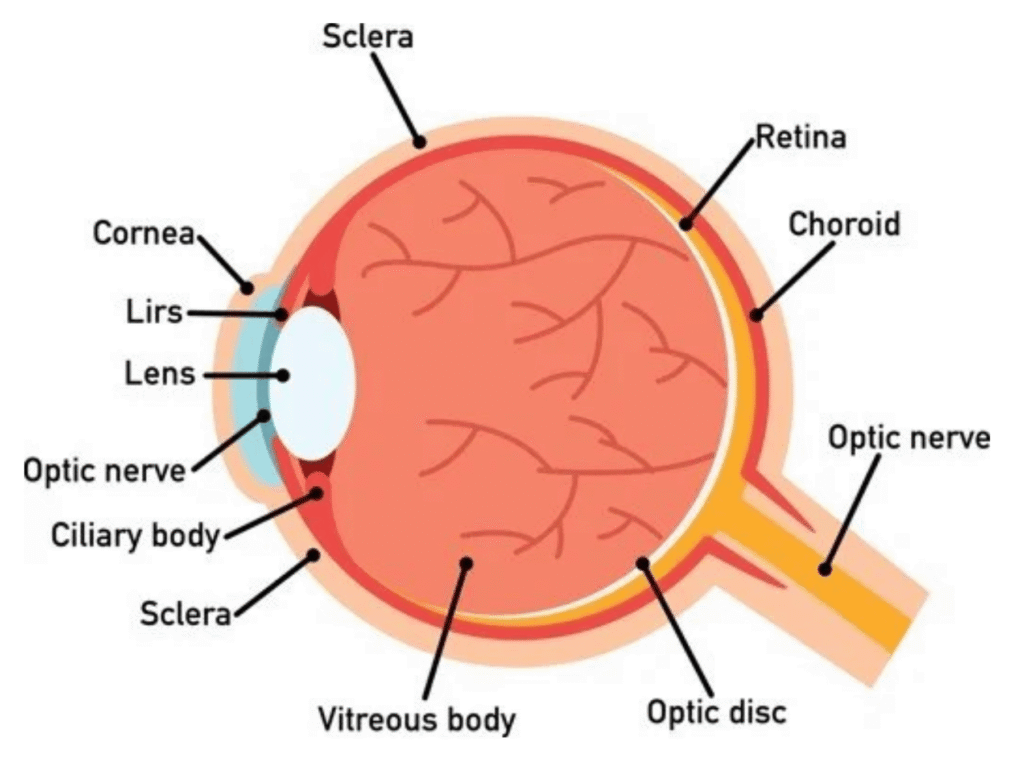
What is the Vitreous?
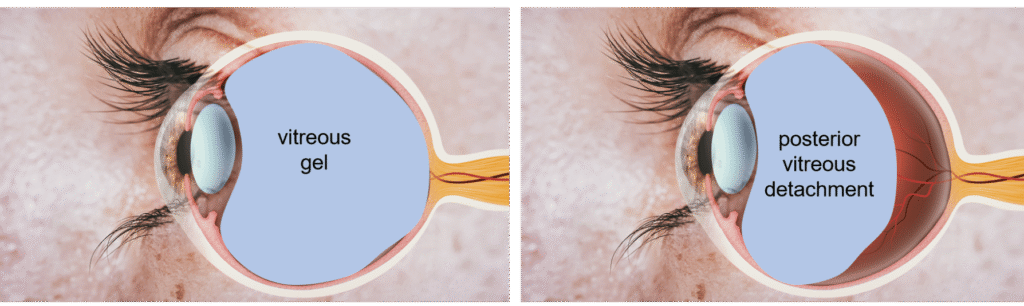
- The inside of the eye is filled with a gel called the “vitreous”
- At birth, the vitreous is a formed gel (like jello) and firmly adherent to the retina
What is a Posterior Vitreous Detachment (PVD)?
- With age, the vitreous gel shrinks and becomes increasingly liquified
- Eventually, the back edge of the vitreous pulls away from the retina to which it was previously adherent. This separation event is called a “posterior vitreous detachment” (PVD)
- PVD is a normal process of aging and occurs in most everyone, eventually (usually in one’s 50s or thereafter)
- Some patients experience no symptoms from their PVD, while others may notice flashes, floaters, or decreased vision
If you have new floaters, new flashes, a curtain in the vision, or decreased vision, a prompt dilated retinal examination is required to evaluate for potential vision-threatening complications of the PVD process
Problems that Can Occur During the PVD Process
- As the vitreous pulls away from the retina, it may be unusually adherent in some areas, tugging on the retina
- Vitreous hemorrhage
- If a blood vessel is tugged on, some bleeding may occur, which can cause lots of floaters or blurry vision or loss of vision
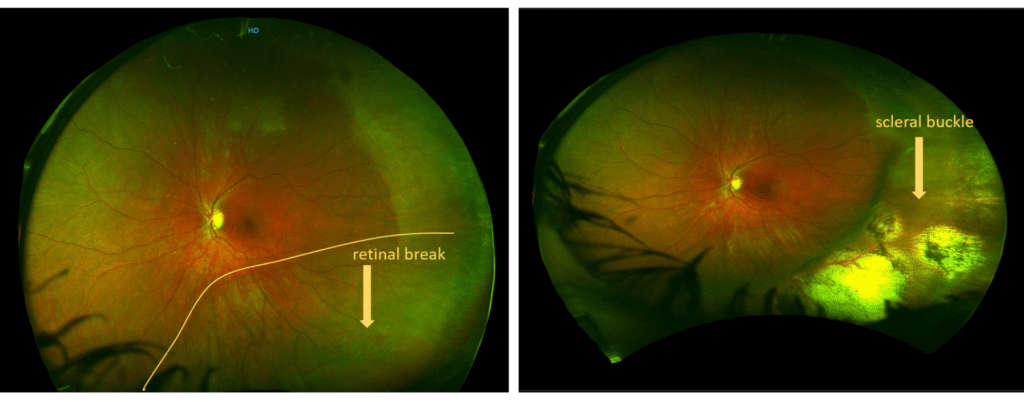
- Retinal tear
- As the vitreous gel tugs on the retina, it can tug hard enough to tear the retina (“retinal tear”)
- Up to 14% of patients with symptoms from a PVD may have a retinal tear
- While the risk is highest at the first visit, there is an increased risk of new tears developing subsequently, especially the first 6-8 weeks after the PVD symptoms began
- As the vitreous gel tugs on the retina, it can tug hard enough to tear the retina (“retinal tear”)
- Retinal detachment
- Without treatment, up to 50% of retinal tears result in retinal detachment
- A retinal detachment occurs because fluid enters through the retinal tear, allowing the retina to detach from the eye wall.
- As an analogy, consider a tear in the wallpaper of the bathroom. If the tear is left unfixed, steam from the shower will eventually cause the entire wallpaper to start peeling off
- Retinal detachment results in vision loss, initially in the peripheral vision and then progressing to involve the central vision

Treatment of a Retinal Tear
- Treatment of a retinal tear reduces (but does not eliminate) the risk of progression to retinal detachment
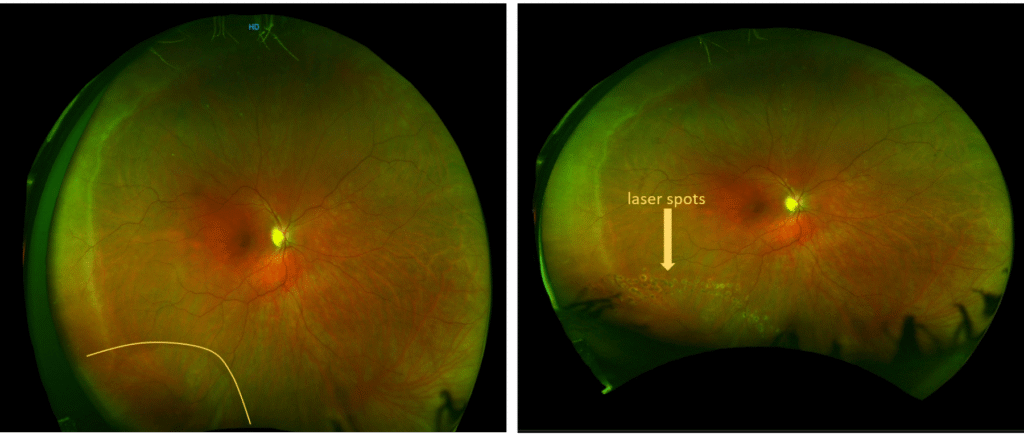
- Treatment involves laser (or less commonly, cryotherapy). The laser treatment is applied in the office, with no need for anesthesia other than topical drops, by special equipment that shines a light into the eye (similar to what happens during the eye exam) and then allows placement of laser spots in the area of concern
- Laser seals the retina surrounding a tear to the eyewall, such that the retina cannot easily detach in that area (like tacking down the retina surround the tear)
- Laser does not eliminate the tear. Laser does not eliminate or change symptoms of flashes or floaters. Laser reduces but does not eliminate risk of the tear progressing to retinal detachment. Laser does not eliminate the risk of future tears occurring elsewhere in the retina.
- Most patients can return to their usual activities after laser is performed, and close followup is performed for the weeks that follow to monitor for progression to retinal detachment, new tears, etc.
Treatment of a Retinal Detachment
- Retinal detachments may be treated in one of several ways, depending upon the specific anatomy and other considerations
- Pars plana vitrectomy
- Micro-incisional surgery whereby the vitreous pulling on the retina is removed, the fluid is drained from under the retina and the retina reattached, and then the tears are treated with laser.
- The laser is like glue such that it takes time to “dry.” Thus, either a gas bubble or an oil bubble is placed in the eye to hold the retina in place while the laser “dries.” Patients cannot see well through the gas (and to some extent, also with the oil bubble). The gas resolves slowly on its own over 3-8 weeks. Oil required a second surgery for removal 3 or more months later.
- Usually, the patient will need to position the head in a specific way (for example, “face down”) for 5-10 days to ensure the gas or oil bubble is supporting the retinal breaks
- Pars plana vitrectomy

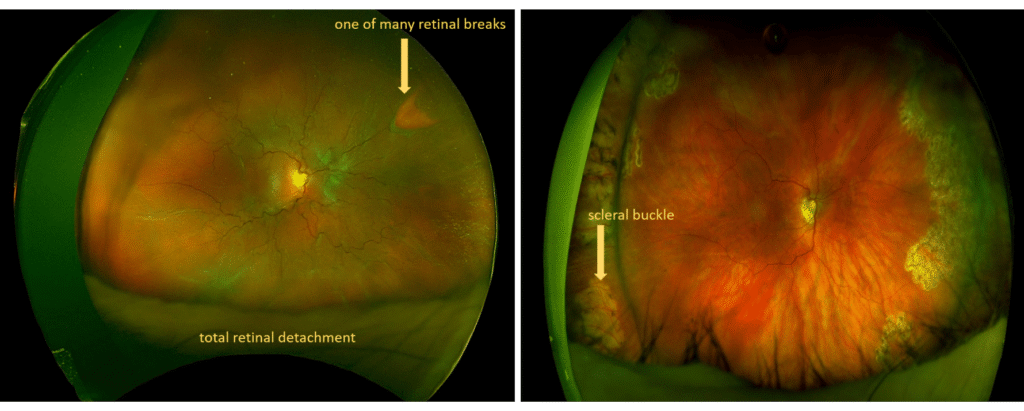
Scleral Buckle Surgery
- A silicone band or implant is affixed to the outside of the eye to support the retinal breaks so that fluid does not continue to track under the retina from the breaks
- The fluid under the retina is either drained to reattach the retina during this surgery or the fluid is allowed to drain on its own over time
- An air gas bubble may or may not be placed in the eye for further support of retinal breaks
Combination surgery with both scleral buckle and pars plana vitrectomy
- Pneumatic retinopexy
- In some cases, the retinal detachment can be repaired by injecting a gas bubble in the eye in the office. With diligent head positioning, the gas bubble can “plug” the retinal break and allow the retina to reattach. Laser can then subsequently be applied to seal the retinal break.
- Laser barricade
- The retina is not reattached but rather a barrier of laser is placed to tack the retina down at the edge and reduce risk of progression